WORKING ON-CALL
2303 - ACCESS CODE FOR EMERGENCY ENTRANCE IN ATRUM (sliding door to left of revolving doors)
You will want this when returning to Brunel building overnight (e.g. having visited CDS)!
Out-of-hours there are 4 non-consultant anaesthetists on site:
-
1st on (9031)
-
2nd on (9032)
-
3rd on (9033/9030)
-
Obstetrics (9035)
Handover
Unless in theatre with a case, handover happens as follows:
-
Morning – 0745hrs in the Anaesthetic Department
-
Evening – 2000hrs in the Anaesthetic Department
-
1st on takes over in Th5, 2nd on takes over in Th6.
1st on-call
Allocated to a doubled-up list to maximise training opportunities, then tasked as required.
Based in theatre 5 after 1700hrs.
2nd on-call
-
Stroke thrombectomy in interventional radiology – daytime cover is only required if the designated IR consultant is already working (7-day consultant cover is provided 0800-1730hrs).
-
Cover 2nd emergency theatre – in practice this often means doing mainly neuro cases in Th6.
-
Be flexible and support where required as requested by 3rd on – you may be asked to go to obstetrics if needed, so it is essential that you have familiarised yourself with the unit before your first on-call.
3rd on-call
Trauma Calls
You are expected to go to trauma calls. ICU also attend. You will always be doubled up in the daytime to allow for this. Trauma calls are run by a Trauma Team Leader (TTL Consultant) who is based in ED.
As a rule of thumb, if a trauma patient is going to theatre, then the 3rd on takes ownership, and if going straight to ICU then ICU take ownership. In reality, it is more dynamic and depends on many factors. Likewise, Consultant involvement is dynamic but as always, call for help if unsure
Obstetric Emergencies
During the day there is a consultant on CDS, but after hours you should respond to these. Code red (major haemorrhage) obstetric calls go to the 3rd on bleep. You will also be called if a 2nd obstetric theatre is needed, or if the obstetric trainee is in theatre and an epidural needs to be done.
As 3rd on-call you should have an overview of how busy the rest of the hospital is and are most likely to be free to respond quickly. Depending on the complexity of cases being done in main theatres, if it is more appropriate, you can send the 1st (if they are obs competent) or 2nd on to obstetrics.
If main theatres is busy, please contact the Obstetric on-call to keep them informed. They can liaise with CDS to ensure that cases are managed appropriately during busy periods.
Coordinating & supportive / supervisory role
Consider the skill mix of the whole on call team at the beginning of the shift and use the other on call tiers working with you to manage the requirements of the on-call.
-
1st on-call can be trainees new to anaesthesia having just passed their initial assessment of competencies to junior registrars. May be able to do obstetrics, but may not.
-
2nd on-call can be junior registrars to ST7 if they need more neuro cases.
-
Obstetric on-call will range from "brand new to obs" to exceptionally experienced staff grades. Please contact the Obstetric on call at the beginning of the shift to establish how busy it is and ensure they know who to contact if they need help.
Use your team according to the skill mix
If you are with a trauma patient, and support is required in obstetrics you may need to ask the 1st or 2nd on to go to Obs. There is no hard and fast rule, use your clinical judgement to decide who should go where E.g. Stable ventilated trauma patient going to scan vs obstetric haemorrhage or failed intubation – may be more appropriate for you to go to obstetrics and for 1st or 2nd on to take over from you. It may also be appropriate to call the consultant if the skill mix or emergency requirements need more senior assistance.
Calling the on-call Consultant
If you need senior advice/support
If workload exceeds resources
-
2 emergency theatres running + receive trauma call à on call consultant should be made aware
-
3rd emergency theatre required à 1st on consultant called in
Obstetrics
The doctor in training is on from 8am until 8:30pm, (30 minutes for hand over) handing over to the night shift who arrives at 8pm (until 8:30 am). On-call is 1 in 8 and is covered by a trainee and consultant/specialist during the daytime (Monday to Saturday). There is a second consultant for elective Caesarean Section lists (weekdays only) and possibly an advanced doctor in training.
After 5.30pm the doctor in training will be supervised (indirectly) by the 3rd on anaesthetic doctor in training and the 1st oncall consultant. There is an additional consultant oncall in the evenings, overnight and at weekends. The names of on-call consultants can be found on the CLW rota and contacted via switchboard. Check who it is at the start of your shift. Please make contact either the 3rd on call DiT, or consultant on call at the beginning of your shift to discuss acuity on CDS. If you have any concerns during your shift (patient or work intensity), please contact the on-call team to discuss. We work as a team and are happy to provide support where needed.
Epidural Level 1 code 700
Level 2 code 855
Remi PCA codes 9035 and 1001
Need to talk about your shift?
Contact your educational supervisor, the consultant you were on call with, or one College Tutors. Please don’t leave it too late after the event. We are here to help.
Other useful information
Consultant Cover
-
Day time, one coordinating consultant, with no theatre responsibilities (9030).
-
After 6pm, general on-call consultant. They expect to be called and will carry 9030 until they leave.
-
From 6-9pm a “third consultant from the senior rota” to help with over-runs, sickness, covering third sessions, etc.
-
From 9pm a “second on” consultant anaesthetist.
-
At weekends an orthopaedic trauma list will run all day Saturday and Sunday (8-5) covered by a consultant anaesthetist from the “senior” rota.
-
At weekends a plastics trauma list will run from 8am – 1pm covered by a consultant anaesthetist on the “senior” rota. This sometimes has extra cover until 5pm too.
-
At the weekends there is a ‘Stroke’ on call consultant anaesthetist who cover 8-5pm. However, the service is 24 hour, so the on call team cover stroke thrombectomies after 6pm.
-
CDS – We have resident cover provided by our Specialist Anaesthetists on Saturdays 8am-6pm.
ICU
-
Four 12 bedded “pods”: A, B, C, D
-
Staffed by doctors in training of varying experience – not all airway competent
-
2 ICU registrars; at least one of which is an anaesthetist
-
ICU Consultants – 4 daytime pod consultants (7 days per week), a 5th Consultant who carries the referral phone during the day on weekdays and 3 on call consultants overnight.
CT Scans for ICU patients – ICU generally do their own scan transfers. If they are short staffed or very busy, they may ask for anaesthetic help, and if we have capacity we should help. If two emergency theatres are running, this may not be appropriate.
ICU Bleeps:
9036 - SHO, who carries the grab-bag to the arrests
9037 - Referrals Registrar
9039 - 2nd Reg (goes to trauma calls when available)
41499 - Consultant for referrals
Cardiac Arrests
ICU attend 24/7, except for the occasional night shift when there is a med reg on the ICU rota and the airway reg is busy (or on a transfer), at which time the ICU team will liaise with anaesthesia teams to ensure that the arrest bleep is covered by the first-on anaesthetist.
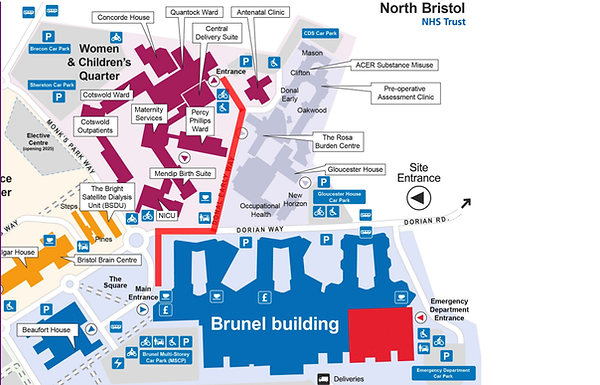
Getting to CDS
Getting to CDS involves leaving Brunel. Out-of-hours the main entrance is locked, but if you follow the glass wall round to the right you will see the “ambulance entrance” where there is a sliding door from which you can exit.
To get back in, there is a keypad (2403) or use the call bell where security will buzz you in.
To get to CDS, either follow the footpath past the Willow cafe and up the road bearing left OR using the back door near the NICU entrance/car park. walking across to the roundabout. There are pink signs you can follow. The route is shown in red on the map below.
It is essential that you have familiarised yourself with CDS before your first on call because if you are obs competent, you may be asked to help.
On-call rooms
There are no dedicated on-call rooms in the Brunel building, but there are on call rooms available on a first come, first served basis. They are rooms adjacent to the doctors’ mess on Level 4. The rooms can only be locked from inside, spare linen is available.
The department has purchased two sleeping pods that have been erected in the department, and there is a sofa bed in the Horfield Room. The Horfield room is a trust meeting room and should be returned to an appropriate state after use. (Please take all linen and scrubs to the linen trollies which are available either as you enter the office complex, or in the changing rooms.
There is a dedicated room on CDS for the obstetric anaesthetist.